

Dose-response in antipsychotics
- Dose-response relationships of antipsychotic drugs for schizophrenia are important in helping clinicians make decisions when prescribing medications.
- Dose-response analysis is based on empirical data, instead of licensed dose ranges.
- Dosing for each patient should still be guided by the properties of each drug, the patients’ characteristics, and the potential interactions of concomitant treatments.
- Higher than currently licensed doses in some drugs can be tested in further trials, since their dose-response curves did not plateau.
In this section
This study by Leucht et al. examines the dose-response relationships of antipsychotic drugs for the acute treatment of schizophrenia and highlights the need for clinicians to follow the minimum and maximum effective doses (which guidelines attempt to provide). During drug development, studies help provide information about dose-response relationships, however these studies may over- or underestimate the maximally effective dose. Indeed doses may be estimated to be too high (i.e., due to toxicity) or too low, hindering further studies to be conducted with higher or lower doses. By contrast, this meta-analysis aims to identify 95% effective doses based on dose-response curves. Leucht and colleagues explore whether higher or lower doses than the currently licensed ones might be more appropriate, and finally derive dose equivalencies from the 95% effective doses (ED95).
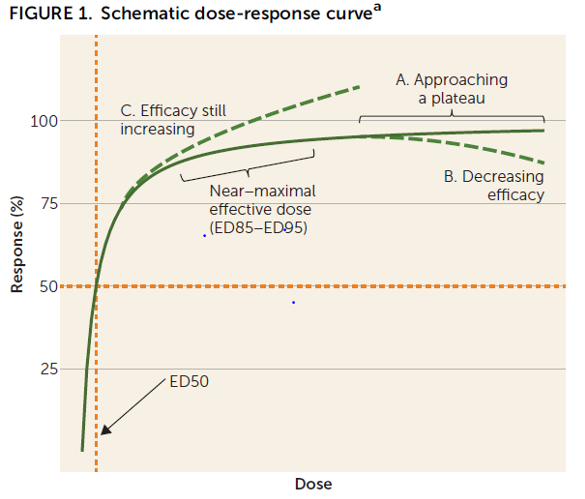
Multiple electronic databases were searched for all placebo-controlled dose-finding studies (68 studies met the inclusion criteria) for 20 second-generation antipsychotics and haloperidol in patients with acute schizophrenia symptoms. Positive and Negative Syndrome Scale (PANSS) and Brief Psychiatric Rating Scale (BPRS) score changes from baseline were measured and 95% effective doses were identified. Dose-response curves were used to identify the ED95, as is customary in dose-response analyses.
Three types of dose-response curves were observed, one plateauing, one decreasing and one increasing.
In the dose-response curves that plateau, such as with cariprazine, higher than currently licensed doses do not need to be tested in further trials, as the efficacy will not increase significantly.
For some drugs, such as risperidone or aripiprazole, the upper limits of licensed doses were found to be higher than the maximum effect doses; the maximum licensed doses of aripiprazole (30 mg/d) and risperidone (16 mg/d) were much higher than the ED95s for these medications (11.5 mg/d and 6.3 mg/d, respectively).
For some of the evaluated antipsychotics, drug-response curves showed bell shapes, meaning a drop in efficacy after plateau. This is most likely due to side effects like extrapyramidal symptoms, which may have continued to increase with the higher doses and may have mimicked negative symptoms and contributed to higher PANSS scores.
For other drugs, such as olanzapine or paliperidone, the dose-response curves were still increasing, suggesting that their ED95 may be higher than the highest doses tested thus far.
| Dose-response curves that plateaued | Dose-response curves that decreased | Dose-response curves that increased |
| Aripiprazole LAI (lauroxil) Asenapine Brexpiprazole Cariprazine Quetiapine | Amisulpride (positive symptoms) Amisulpride (predominant neg. symptoms) Aripiprazole oral Haloperidol Olanzapine (predominant negative symptoms) Risperidone oral Risperidone LAI | Iloperidone Lurasidone Olanzapine oral (positive symptoms) Olanzapine LAI Paliperidone oral Paliperidone LAI Sertindole Ziprasidone Clozapine* *Cautious interpretation is advised because there were only 2 data points and because the small sample size was small (n=48) |
Furthermore, Leucht and colleagues used the ED95s to calculate risperidone, olanzapine, and haloperidol dose equivalence ratios for all examined drugs.
Table 1: Dose equivalencies for antipsychotic drugs
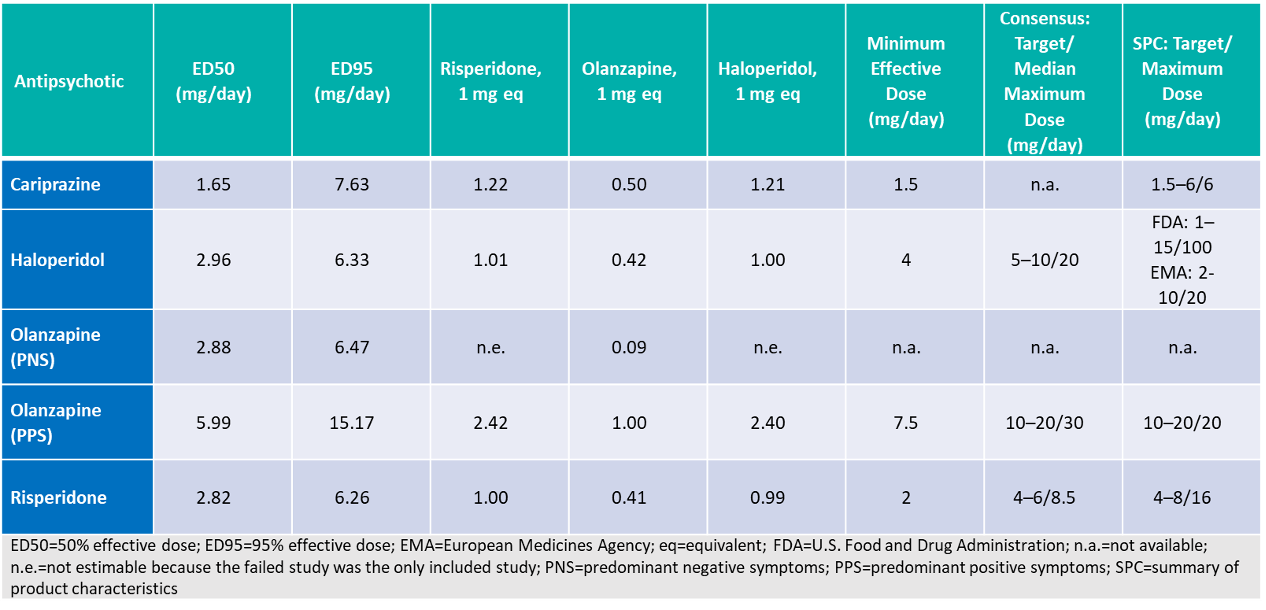
Overall, the results of this study point out that some antipsychotic drugs still have room to be more efficacious than their currently licensed doses, while some are used in higher doses than needed. Concerning cariprazine, the dose-response curve plateaued, emphasising that the licensed doses are adequate and higher doses would not necessarily lead to higher efficacy.
Cod: 300021/R49. Submitted to AIFA on 26/10/2021
References
- Leucht S, Crippa A, Siafis S, Patel MX, Orsini N, Davis JM. Dose-Response Meta-Analysis of Antipsychotic Drugs for Acute Schizophrenia. Am J Psychiatry. 2020; 177(4):342-353. doi:10.101176/appi.ajp.2012.19010034
Am J Psychiatry
Dose-Response Meta-Analysis of Antipsychotic Drugs for Acute Schizophrenia
Abuso de sustancias y psicosis Abuso de sustancias y psicosis
La psicosis es un problema de salud mental que hace que temporalmente la persona afectada interprete la realidad de manera diferente a quienes la rodean. Se La psicosis es un problema de salud mental que hace que temporalmente la persona afectada interprete la realidad de manera diferente a quienes la rodean. Se
Leer másREAGILA en la esquizofrenia aguda Nuestro producto en la esquizofreni...
Una vez establecido el diagnóstico de esquizofrenia, los médicos, los pacientes y las familias tienen que tomar importantes decisiones. Aunque parece de Una vez establecido el diagnóstico de esquizofrenia, los médicos, los pacientes y las familias tienen que tomar importantes decisiones. Aunque parece de
Leer más